What Healthcare Practices Should Know About CMS & Medicare Updates in 2026
- Med Cloud MD
- Jan 28
- 7 min read

Updated: Feb 8
Quick Summary for Providers: CMS has released major Medicare updates for 2026 affecting physician payments, telehealth rules, and billing compliance. The Physician Fee Schedule includes a 3.26% increase for most providers, permanent telehealth changes, new prior authorization requirements, and significant adjustments to practice expense calculations. These changes directly impact your reimbursement, cash flow, and billing operations starting January 1, 2026.
If you bill Medicare, 2026 brings some of the most significant changes to physician payments and compliance requirements in years.
The Centers for Medicare & Medicaid Services just finalized multiple rule changes that'll affect how you get paid, what documentation you need, and which services require prior authorization. Some changes help practices like the first real payment increase in years. Others create new billing headaches.
Most providers I talk to haven't dug into these updates yet. That's a problem, because ignorance won't protect you from claim denials or audit risks once these rules take effect January 1st.
This guide breaks down what actually matters for your practice: the payment changes, new telehealth rules, billing compliance updates, and how to avoid the denial traps built into these new regulations.
Understanding the 2026 Medicare Physician Fee Schedule Changes
The Physician Fee Schedule is how Medicare determines what they'll pay you for professional services. Every year, CMS adjusts these rates, and 2026 brings some notable changes.
The Payment Increase
After years of cuts and flat payments, Congress approved a temporary 2.5% increase for 2026. Combined with other statutory adjustments, most physicians will see conversion factors rise by about 3.26%.
If you participate in Advanced Alternative Payment Models (APMs), your increase is slightly higher 3.77%.
Here's what that means in dollars:
The conversion factor for non-APM participants: $33.40
The conversion factor for APM participants: $33.57
Sounds good, right? Not so fast.
The Catch: Practice Expense and Efficiency Adjustments
While the conversion factor went up, CMS also adjusted practice expense calculations and applied efficiency adjustments to many codes. These changes redistribute payments across specialties and practice settings.
Who gets hit hardest:
Hospital-based physicians (11% average cuts for some specialties like hematology/oncology)
Physicians billing certain procedural codes
Practices in facility settings versus non-facility settings
Who benefits:
Community-based practices
Primary care providers
Certain evaluation and management services
The net result? Some physicians will actually see payment decreases despite the overall rate increase. You need to check how your specific CPT codes were affected.
Telehealth Changes You Need to Know
Telehealth rules have been in flux since the pandemic. CMS finally made several changes permanent for 2026.
What's Now Permanent
Frequency limitations removed: You can now bill for subsequent inpatient visits, nursing facility visits, and critical care consultations via telehealth without frequency limits.
Virtual direct supervision: For services requiring direct supervision, physicians can now supervise via real-time audio and video permanently. No more physical presence requirements for certain services.
Permanent telehealth codes: Select audiology and speech-language pathology codes are now permanently on the Medicare Telehealth Services List.
The Home Address Issue (Resolved)
CMS initially proposed requiring all physicians providing telehealth from home to list their home addresses in the Medicare enrollment database. After massive pushback, they clarified:
You DON'T need to report your home address if:
You have another practice location already enrolled in Medicare
You only occasionally provide telehealth from home
You DO need to report it if:
Telehealth from home is your primary practice
You have no other enrolled practice location
Even if you must report a home address, you can suppress street details so patients and the public only see your city and state.
What's Still Temporary
Medicare telehealth authority for some providers was only extended through January 30, 2026. Unless Congress acts again, you could lose telehealth billing rights mid-year.
This uncertainty makes long-term planning difficult for telehealth-heavy practices.
Medicare Advantage and Part D Updates
If you treat Medicare Advantage patients, several rule changes affect how plans operate and pay providers.
Prior Authorization Restrictions
CMS finalized a provision restricting MA plans' ability to reopen and modify previously approved inpatient hospital decisions based on information gathered after approval. Under this rule, MA plans can only reopen approved admissions for obvious error or fraud.
What this means: When an MA plan approves an inpatient admission, they have to honor it. They can't retroactively deny payment because they decided later the admission wasn't necessary.
This is a huge win for hospitals and physicians tired of fighting retroactive denials.
Improved Provider Directory Requirements
MA plans must now submit provider directory data to CMS for online publication. If a plan becomes aware of a data change, they must update CMS within 30 days.
This should reduce patient frustration from inaccurate directories, but it also means you need to notify your MA plans promptly when your information changes.
Prescription Drug Payment Plan
All Medicare Part D plans must now offer enrollees the option to spread out-of-pocket drug costs over monthly payments instead of paying everything at the pharmacy.
While this helps patients afford medications, it creates administrative complexity for practices that bill and collect for physician-administered drugs.
What These Changes Mean for Medical Billing
CMS updates don't just affect what you get paid they change how you have to bill.
Clean Claim Submission Just Got Harder
With practice expense adjustments and efficiency factors applied to specific codes, your billing team needs updated fee schedules and code-specific guidance.
Common billing mistakes to avoid:
Using outdated fee schedules from 2025
Failing to verify which conversion factor applies (APM vs non-APM)
Not adjusting for place-of-service changes affecting practice expense
Missing new modifiers required for certain telehealth services
Documentation Requirements Are Tighter
CMS continues emphasizing documentation quality, especially for evaluation and management services and behavioral health integration.
What you need now:
Clear medical necessity documentation for all services
Proper time documentation for time-based codes
Compliance with new telehealth documentation standards
Updated policies reflecting 2026 supervision requirements
Prior Authorization Expansion
CMS is implementing mandatory prior authorization models for certain services and geographies, including skin substitutes and specific high-cost items.
If you're in an affected geography, claims for these services without prior authorization will be automatically denied starting in 2026.
Compliance Risks Practices Are Missing
Every CMS update creates new audit targets. Here's what's on their radar for 2026.
Skin Substitute Billing Changes
CMS is cracking down hard on skin substitute billing. The agency notes spending on these products increased from $252 million in 2019 to over $10 billion in 2024.
New payment methodology sets a single rate around $127 for skin substitutes, drastically lower than previous reimbursements. Expect intense scrutiny of medical necessity documentation and prior authorization compliance.
Telehealth Supervision Audits
With permanent virtual supervision rules, CMS will audit whether physicians actually provided real-time audio-visual oversight when they billed for supervised services.
You need documentation proving:
Audio-visual technology was used
The supervising physician was immediately available
Communication occurred during the service
Practice Expense Documentation
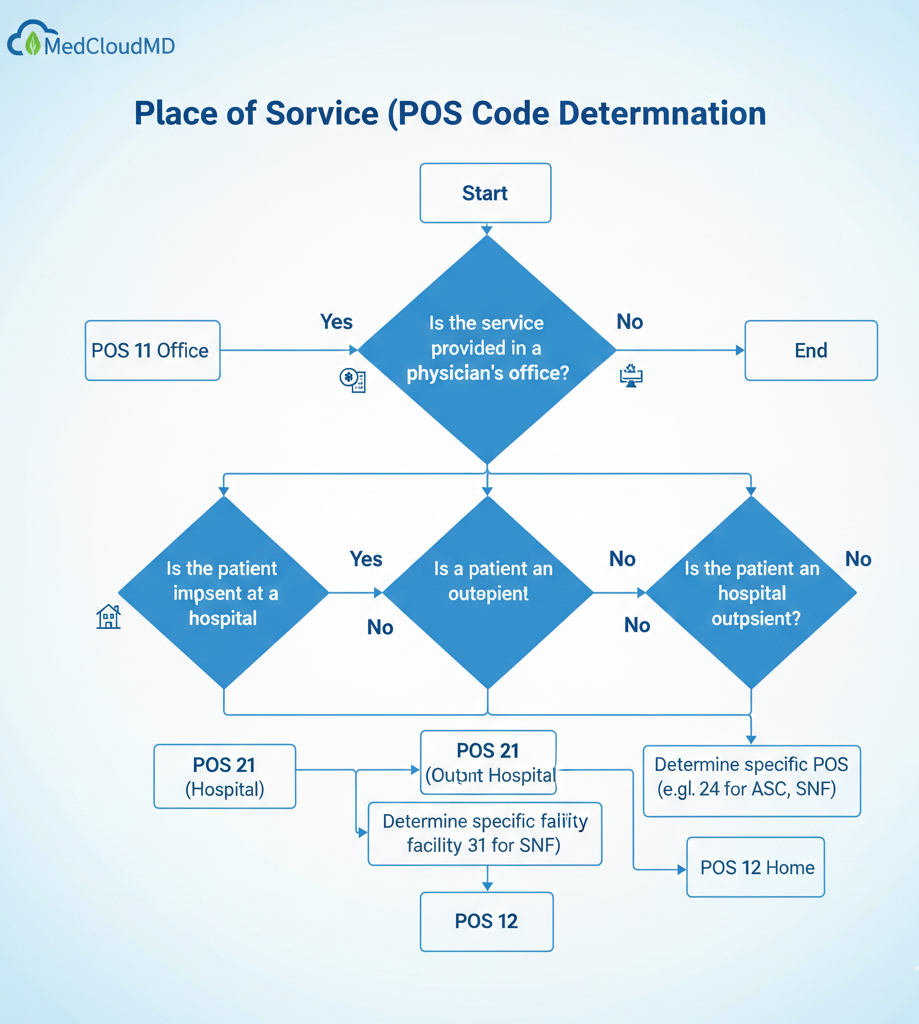
The practice expense calculation changes mean CMS will compare facility versus non-facility billings more carefully. Billing the wrong place of service code now has bigger financial implications.
How MedCloudMD Keeps Practices Compliant
Staying on top of CMS updates while running a medical practice is nearly impossible. That's where MedCloudMD's revenue cycle management expertise makes a real difference.
We Monitor Every CMS Change
Our compliance team tracks every final rule, transmittal, and MLN Connects update. We update our billing systems, fee schedules, and coding protocols immediately when changes take effect.
You don't have to wade through hundreds of pages of Federal Register documents. We translate complex regulations into actionable billing procedures for your practice.
Specialty-Specific Billing Expertise
Different specialties are affected differently by CMS changes. Our billing specialists understand how 2026 updates impact cardiology practices, behavioral health providers, and urgent care centers specifically.
We adjust coding, documentation requirements, and claim submission workflows based on your specialty's unique needs.
Proactive Denial Prevention
Our AI-powered claim scrubbing catches compliance issues before claims submit. We verify:
Correct conversion factors are applied
Place of service codes match the service provided
Prior authorization is obtained when required
Documentation supports medical necessity under 2026 standards
This proactive approach keeps denial rates low and cash flow steady even when regulations change.
Real-Time Fee Schedule Updates
The moment CMS releases updated fee schedules, we implement them across all claims. You never risk underbilling or overbilling because of outdated rates.
Our transparent reporting shows exactly what you're being paid versus what you should be paid, making it easy to spot underpayments and file corrective claims.
Learn more about our denial management services →
Frequently Asked Questions
How will the 2026 Medicare payment increase affect my practice?
Most providers will see a 3.26% conversion factor increase, though actual payment changes vary by specialty and practice setting due to practice expense adjustments. Hospital-based specialists may see decreases while community-based primary care typically sees increases. Review your specific CPT codes to determine your practice's impact.
Do I need to report my home address to Medicare if I provide telehealth services?
Only if telehealth from home is your primary practice and you have no other enrolled practice location. If you have another practice location enrolled, you can continue using that address even if you occasionally provide telehealth from home.
What happens if Medicare Advantage plans deny claims I already have prior authorization for?
Under 2026 rules, MA plans can only reopen previously approved admissions for obvious error or fraud. If they retroactively deny an authorized service for other reasons, you have strong grounds for appeal. Document all prior authorizations carefully.
How do I know if my specialty is affected by the practice expense changes?
Review the CMS Physician Fee Schedule final rule or consult with your billing team. Generally, hospital-based procedural specialties saw cuts while community-based evaluation and management services saw increases. Your Medicare Administrative Contractor can provide specialty-specific impact data.
Are telehealth services still covered by Medicare in 2026?
Many telehealth flexibilities are now permanent, including virtual direct supervision and certain services on the permanent telehealth list. However, some provisions were only extended through January 30, 2026, and require congressional action to continue beyond that date.
What documentation do I need for virtually supervised services?
You must document that real-time audio-visual technology was used, the supervising physician was immediately available during the service, and actual communication occurred. Virtual supervision cannot be used for services requiring physical presence for patient safety.
How does the skin substitute payment change affect my practice?
If you use skin substitutes, Medicare now pays a single rate around $127 regardless of product. Many geographies require mandatory prior authorization. Medical necessity documentation must be thorough, as this is a high-audit-risk area for CMS in 2026.
Don't Let CMS Updates Derail Your Revenue
CMS regulatory changes happen every year, but 2026 brings more significant shifts than usual. Payment methodology changes, permanent telehealth rules, and new compliance requirements all affect your revenue cycle operations.
The practices that handle these transitions smoothly have one thing in common: they partner with billing experts who make compliance and regulatory updates someone else's problem.
At MedCloudMD, we've already updated our systems for every 2026 change. Our clients' claims are submitting with correct fee schedules, proper documentation, and full compliance because we handled the heavy lifting.
You shouldn't have to become a CMS regulations expert to get paid correctly. That's our job.



Comments